Atlantoaxial Instability (AAI) in People with Down Syndrome
May 20, 2025
Key Points
- Atlantoaxial instability is abnormal movement between the first and second vertebrae (bones) in the neck.
- Atlantoaxial instability is much more common in people with Down syndrome compared to people without Down syndrome.
- Depending on the amount of abnormal movement in the neck and a person’s symptoms, treatment may include monitoring with regular exams and perhaps imaging (such as x-rays or MRI). When there are symptoms, surgical repair is usually recommended.
- In the United States, both the pediatric and adult medical care guidelines for people with Down syndrome recommend screening for atlantoaxial instability regularly through a good history and physical exam by a health care professional. Neither recommends screening x-rays for people with Down syndrome who do not have symptoms of atlantoaxial instability.
- Caution to prevent spinal injury is recommended whenever a person with Down syndrome undergoes anesthesia (whether they do or do not have atlantoaxial instability).
What is atlantoaxial instability?
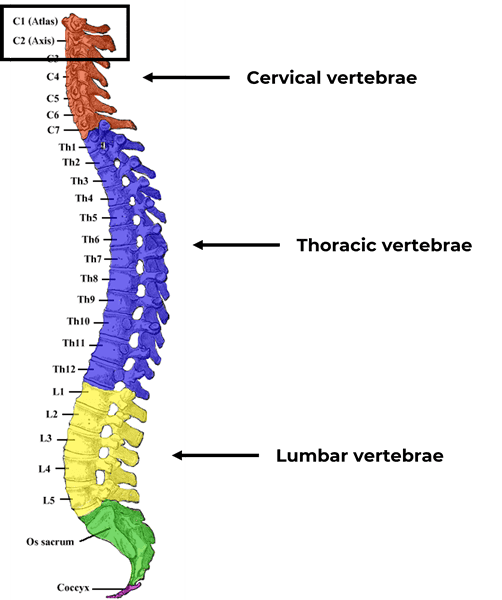
Atlantoaxial instability, also referred to atlantoaxial subluxation, is abnormal movement between the first and second vertebrae in the neck. The condition is sometimes called C1-C2 instability.
- Cervical vertebrae – vertebrae (bones) in the neck
- C1 – first vertebra, also called the atlas
- C2 – second vertebra, also called the axis
Atlantoaxial instability falls under the broader category of spondylolisthesis, which is a slippage of one vertebra over another. It can cause the spine or adjacent nerves to be compressed by the vertebrae, ligaments, or other tissues. This slippage or instability may occur anywhere in the spine, including any of the cervical and lumbar vertebrae. It can occur in the thoracic vertebrae but that is less common. Spondylolisthesis can also occur at the joint between the base of the skull and the top of the spine.
Symptoms
Atlantoaxial instability can cause many symptoms including:
- Pain in the neck or head
- Holding the head in unusual positions
- Not wanting to or being unable to move the head and neck
- Difficulty holding the head up
- Weakness of the arms and/or legs
- A person may drop objects, have difficulty buttoning a shirt, appear to be clumsy, have impaired balance, walk unsteadily, lean to the side while walking, etc.
- Incontinence of urine and/or stool (e.g., having bathroom accidents)
- Numbness and/or tingling
- Not wanting to participate in activities
- Abnormal breathing or difficulty breathing
- Nerves that pass through the upper cervical spine stimulate the body to breathe by causing the diaphragm to contract. If the part of the spine where these nerves are present is injured, the body cannot stimulate breathing movements.
- Rarely, the movement of the vertebrae and/or bony growths related to arthritis may protrude anteriorly (forward) causing narrowing of the upper airway and cause swallowing dysfunction.
Some symptoms may affect only one side of the body or both sides.
A person with Down syndrome can develop atlantoaxial instability at any age. Even if a person did not have it when they were younger, they could develop it later in life. Some factors that can contribute to the development of atlantoaxial instability later in life include:
- Deterioration of joints over time, such as with osteoarthritis
- Formation of bony overgrowths (osteophytes)
- Deterioration of the discs between the vertebrae
- Thickening of ligaments
- Fractures
- Tumors
When symptoms occur, weakness or paralysis is a common feature of atlantoaxial instability. Sometimes, the paralysis is reversible with surgery. However, once weakness has occurred, there may be some permanent paralysis. Further damage can usually be prevented and sometimes strength can be regained.
Atlantoaxial instability and Down syndrome
Atlantoaxial instability is much more common in people with Down syndrome compared to people without Down syndrome.
In our study on frequency of conditions experienced by individuals with Down syndrome evaluated in our health system, atlantoaxial instability was present in 2.5% of individuals with Down syndrome. It was 78 times more common in the individuals with Down syndrome in our study compared to the comparison group of individuals without Down syndrome. Other studies have found a much higher frequency in people with Down syndrome (20-30%). Most of the individuals in the studies did not have symptoms. Our frequency is lower because our sample is primarily people with symptoms who have been evaluated and diagnosed with atlantoaxial instability.
Atlantoaxial instability is more common in people with Down syndrome due to differences in the ligaments and connective tissues that connect one bone to another bone and hold the joint between bones together. In people with Down syndrome, because the connective tissue is different, the ligaments are “stretchier,” which tends to make the joints looser. The difference in connective tissue also contributes to problems in multiple other organs in the body.
Screening
Pediatric guidelines
The American Academy of Pediatrics (AAP) recommends regular, periodic screenings to assess for symptoms and physical findings that indicate spine or nerve compression. Their recommendation is:
“Discuss with parents, at least biennially, the importance of cervical spine-positioning precautions for protection of the cervical spine during any anesthetic, surgical, or radiographic procedure. Perform careful history and physical examination with attention to myelopathic signs and symptoms at every well-child visit or when symptoms possibly attributable to spinal cord impingement are reported. Parents should also be instructed to contact their physician for new onset of symptoms of change in gait or use of arms or hands, change in bowel or bladder function, neck pain, stiff neck, head tilt, torticollis, how the child positions his or her head, change in general function, or weakness.”
Adult guidelines
The Global Down Syndrome Foundation Medical Care Guidelines for Adults with Down Syndrome (“Global Adult Guidelines”) make a similar recommendation regarding annually assessing for symptoms and physical findings for spine and nerve compression. Additionally, the Global Adult Guidelines add:
“While avoiding potential SCI (spinal cord injury) is important, restricting asymptomatic individuals with AAI (atlantoaxial instability) from participating in physical activities is also undesirable for reasons related to physical and psychological health. Additional indirect evidence has suggested that SCI from AAI is uncommon.”
In the past, periodic neck x-rays were recommended to screen for atlantoaxial instability before sports or before anesthesia for surgery. However, that is not the recommendation of the AAP or Global Adult Guidelines. Special Olympics required x-rays in the past for all people with Down syndrome to participate. The United States (national) Special Olympics form requires a history and physical exam to assess for symptoms and signs of spinal cord compression but not neck x-rays. This change is being phased into each state’s Special Olympics requirements.
Diagnosis
A health care professional takes a history assessing for the symptoms described above. The professional also performs a physical exam that should include checking for:
- Increased deep tendon reflexes – done by tapping with the reflex hammer.
- Clonus – a repetitive movement of the feet and/or hands found by extending the wrist or ankle with gentle force.
- Abnormal plantar reflex – the big toe goes up when stroking the bottom surface of the foot.
- Muscle weakness.
Additional diagnostic testing may include:
- Neck x-rays – these are lateral x-rays (taken from the side). They are taken with flexion (the person gently bending their head forward), extension (the person gently bending their head backward), and neutral position.
- Magnetic resonance imaging (MRI) – assesses the spinal cord for evidence of compression or injury.
- Computed tomography (CT) scan – assesses the bone structure.
- Electromyogram (EMG) – this assesses nerve and muscle function and may be done if the diagnosis is not certain based on other testing.
A referral to a neurosurgeon or an orthopedic surgeon may also be made. Depending on the availability of a surgeon in the local community, sometimes a referral to a surgeon in a bigger medical center and/or university might be indicated. Anesthesiologists and physicians assisting with post-operative care who are familiar with providing care for people with Down syndrome can be invaluable.
Prevention
There is no known prevention for atlantoaxial instability in people with Down syndrome. However, there are ways to reduce the likelihood of spinal cord compression due to atlantoaxial instability.
Sports
As noted above, limiting participation in sports for individuals with Down syndrome who do not have symptoms of atlantoaxial instability has a low likelihood of preventing significant injury and has negative implications for physical and psychological health.
However, certain sports or activities are higher risk. Teaching methods to reduce injury is encouraged. For example, in tackle football, avoiding tackling headfirst, using one’s shoulders instead to make the tackle. Avoiding trampoline use or, at minimum, using trampolines only with proper training is recommended by the AAP for all children whether they have Down syndrome or not.
If a person has been diagnosed with atlantoaxial instability, it is typically recommended that they do not play contact sports, dive, tumble, or do the butterfly stroke in swimming.
Anesthesia
During anesthesia for surgery or a procedure, sometimes an endotracheal (breathing) tube is placed in the airway. This may require extending the neck backwards for proper placement. This posterior extension is not recommended for people with Down syndrome whether they do or do not have atlantoaxial instability.
Spinal cord injury may occur even if the person does not have atlantoaxial instability. Therefore, for any person with Down syndrome undergoing the placement of an airway tube, it is recommended that the tube be placed with a scope. This is called fiberoptic visualization and it allows the airway to be viewed without extending the neck backwards.
Inflammatory arthritis
Atlantoaxial instability can also be caused by inflammatory arthritis such as rheumatoid arthritis. Individuals with Down syndrome have higher frequencies of autoimmune conditions. Some of these conditions cause inflammatory arthritis that could contribute to the development of atlantoaxial instability. Appropriate treatment, often with a rheumatologist, is recommended to reduce the inflammation.
Treatment
Observation
Ongoing observation may be recommended for someone with no symptoms and no evidence of spinal cord injury on the MRI. Regular exams and possibly imaging (x-rays and/or MRI) may be ordered.
Surgery
Surgery is usually recommended for someone with symptoms and/or evidence of spinal cord injury or compression on the MRI.
Before or during the surgery, the vertebrae must be adjusted away from the spinal cord and then stabilized so the corrected position is maintained. The spine is often stabilized with rods, screws, and/or a bone graft (often from the hip). Occasionally, a “halo” device is screwed into the skull with 4 screws. It holds the neck stable while it heals. The person may also need several weeks to months of physical and occupational therapy to help regain strength or lost skills. People who had neurologic impairment before the surgery may need physical therapy for several months to optimize function.
If surgery is recommended, we encourage a thorough discussion with the orthopedic surgeon or neurosurgeon. Suggested questions to discuss include:
- What are the indications for surgery? What symptoms or neurological findings indicate surgery is needed?
- What are the risks of surgery?
- How might the individual’s health status affect treatment?
- Can the person physically tolerate surgery?
- Are there other serious underlying health issues that are likely to impact recovery?
- Heart function – particularly if the person had heart problems as a baby (congenital heart disease)
- Swallowing – some individuals have swallowing problems after the operation
- Sleep apnea – sleep apnea is more common in people with Down syndrome and can cause significant problems after surgery
- Alzheimer’s disease – will the surgery provide an improvement or decline in quality of life, might it increase life expectancy or shorten it, will the person be able to tolerate the surgery and/or follow-up care and therapy required?
- Will the person be able to participate in the rehabilitation process after surgery? If not, how will that impact the outcome?
Prognosis
There is a high risk of complications after surgery for atlantoaxial instability in adults with Down syndrome. However, there are also risks if atlantoaxial instability is not surgically repaired. People with progressively symptomatic atlantoaxial instability, are at risk for paralysis, immobility, and even death.
A study by Siemionow et al. published in 2017 reported a high complication rate after surgery for atlantoaxial instability in adults with Down syndrome. Pneumonia was the most common complication in the study. However, the study also reported that a total of 16 of 17 patients (94.1%) demonstrated stabilization or improvement in neurologic status. The authors concluded that this outcome seems to warrant the high complication risk associated with cervical spine surgery in individuals with Down syndrome.
There are ways to increase the likelihood of success of surgery for atlantoaxial instability in adults with Down syndrome. For example, research has shown that using specific surgical techniques can improve the cervical spine outcome in people with Down syndrome. Additionally, high quality care after surgery, particularly by health professionals familiar with caring for people with Down syndrome, can increase success. Choosing a hospital with experience in providing this type of care for people with Down syndrome should be considered. Physical and occupational therapy by therapists familiar with treating people with Down syndrome can also have a significant positive impact on the outcome.
After the person has had the surgery and recovered, they can resume most of their activities. It is generally recommended to continue to avoid the activities that someone with untreated atlantoaxial instability should avoid (contact sports, diving, tumbling, and the butterfly stroke in swimming).
Resources
Adult Guidelines for Families (Global Down Syndrome Foundation)
Alzheimer’s Disease (National Down Syndrome Society)
Are Trampolines Safe for Kids? (American Academy of Pediatrics)
Pediatric Guidelines for Families (American Academy of Pediatrics)
References
Bull MJ, Trotter T, Santoro SL, et al. Health supervision for children and adolescents with Down syndrome. Pediatrics. 2022;149(5):e2022057010. doi:10.1542/peds.2022-057010
Chicoine B, Rivelli A, Fitzpatrick V, Chicoine L, Jia G, Rzhetsky A. Prevalence of common disease conditions in a large cohort of individuals with Down syndrome in the United States. J Patient Cent Res Rev. 2021;8(2):86-97. doi:10.17294/2330-0698.1824
Hofler RC, Pecoraro N, Jones GA. Outcomes of surgical correction of atlantoaxial instability in patients with Down syndrome: Systematic review and meta-analysis. World Neurosurg. 2019;126:e125-e135. doi:10.1016/j.wneu.2019.01.267
Siemionow K, Hansdorfer M, Janusz P, Mardjetko S. Complications in adult patients with Down syndrome undergoing cervical spine surgery using current instrumentation techniques and rhBMP-2: A long-term follow-up. J Neurol Surg A Cent Eur Neurosurg. 2017;78(2):113-123. doi:10.1055/s-0036-1584905
Tomlinson C, Campbell A, Hurley A, Fenton E, Heron N. Sport preparticipation screening for asymptomatic atlantoaxial instability in patients with Down syndrome. Clin J Sport Med. 2020;30(4):293-295. doi:10.1097/JSM.0000000000000642
Tsou AY, Bulova P, Capone G, et al. Medical care of adults with Down syndrome: A clinical guideline. JAMA. 2020;324(15):1543-1556. doi:10.1001/jama.2020.17024
Join our mailing list
Sign up to receive emails with information on health topics for teens and adults with Down syndrome, updates on research and education as well as information about upcoming events, classes and programs.